A clinical score to predict mortality in septic acute kidney injury patients requiring continuous renal replacement therapy: the HELENICC score
Background
본 연구는 continuous renal replacement therapy(CRRT, 지속적 신대체 요법)가 필요한 septic acute kidney injury(패혈증에 병발한 급성 신부전) 환자의 early(7-day) mortality를 예측하는 방법을 알아보았다.
Methods
브라질의 3차 병원에서 2005년 10월부터 2010년 11월까지 중환자실에 입원해서 CRRT를 시행받은 186명의 septic AKI 환자를 대상으로 한 prospective study이다.
Results
Multivariate adjustment 후 다음 5가지의 variable이 primary outcome(early mortality)와 관련 있는 것을 확인할 수 있었다: norepinephrine utilization, liver falire, medical condition, lactate level, pre-dialysis creatinine level
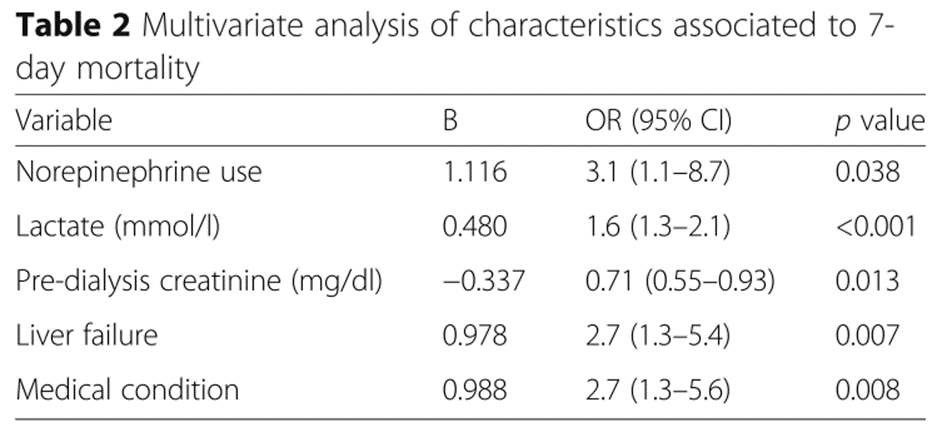
위 varialbe을 조합해서(proportionally to the odds ration for each variable) scoring system을 고안하였다:
(medical condition x 6) + (liver failure x 6) + (norepinephrine x 6) + (lactate x 3) - (creatinine x 2)

이 scoring system은 C-static 0.82(95% CI = 0.76 - 0.88)로 good discrimination 및 good claibration (χ2 = 4.3; p = 0.83)을 보였고, 위 환자군에서 SAPS 3, APACHE II, SOFA score는 poor performance를 보였다.
Conclusions
CRRT를 시행받은 septic AKI 환자에서 HEpatic failure, LactatE, NorepInephrine, medical Condition, and Creatinine (HELENICC) score는 early mortality 예측하는 데 좋은 결과를 보였다. 다른 환자군에서도 이러한 결과가 나오는지 확인하기 위해 추가 연구가 필요하다.
Context
중환자실에 입실하고 24시간 이내에 사망이 예상되는 환자와 CRRT 등의 중환자 치료를 거부한 환자는 연구에서 제외하였다. Acute kidney injury 분류는 Acute Kidney Injury Network(AKIN) criteria에 따랐습니다. Serum creatinine value는 중환자실 입실 후 cumulative fluid balance로 보정하였다.
Macedo 등은 253 명의 중환자를 대상으로 한 전향적 연구에서 fluid accumulation에 의한 creatinine의 dilution이 AKI의 중증도를 과소평가함으로써 creatinine의 상승이 검사에 반영되는 시간을 지연시킬 수 있음을 제시하였다.
Macedo et al. Program to Improve Care in Acute Renal Disease S. Fluid accumulation, recognition and staging of acute kidney injury in critically-ill patients. Crit Care. 2010;14(3):R82.
본 연구에서는 CRRT 시작 당시의 높은 creatinine level이 protective effect가 있는 것으로 나타났는데, 이는 Cerda 등이 관찰한 바와 같다.
Cerda J et al. In severe acute kidney injury, a higher serum creatinine is paradoxically associated with better patient survival. Nephrol Dial Transplant. 2007;22(10):2781–4.
adjusted creatinine = sCr x correction factor.
Correction factor
= (hospital admission weight (kg) x 0.6 + Σ (daily cumulative fluid balance L))) / hospital admission weight x 0.6
Septic AKI는 sepsis와 AKI 둘 다 진단된 경우로 정의하며, sepsis 이외의 다른 원인(i.e., urinary tract obstruction, radio contrast media, other nephrotoxins)에 의해 발병한 AKI는 제외하였다. Comormidity는 중환자실 입실 당시의 ICD-9 code로 확인하였습니다. Medical condition은 중환자실 입실 사유가 내과적 경우(i.e., non-surgical)로 정의하였다.
본 연구에서 수집한 kideny fuction data는 다음과 같다:
sreum creatinine, urea, urine output
환자 상태의 중증도(severity of illness)는 CRRT 시작 당시의 APACHE II, SAPS 3, SOFA score로 확인하였다.
Bagshwa 등은 septic AKI 중환자 군이 non-septic AKI 중환자군에 비해 중증도가 더 높다고 보고하였다:
The severity of illness scores, concomitant non-renal organ dysfunction, need for mechanical ventilation, proportion of patients who required vasoactive therapy, in-hospital case-fatality rate이 더 높았다.
Bagshaw SM et al. Early acute kidney injury and sepsis: a multicentre evaluation. Crit Care. 2008;12(2):R47.
Reference
da Hora Passos et al. BMC Anesthesiology (2017) 17:21
https://blueorbit.tistory.com/294
Acute kidney injury(급성 신부전) 환자에서 투석을 언제 시작하는게 좋을까?
Timing of Initiation of Renal-Replacement Therapy in Acute Kidney Injury BACKGROUND 중환자에서 자주 발생하는 Acute kidney injury(급성 신부전) 환자의 많은 경우 결국 투석을 필요로 하게 됩니다. 하지만 투석을 언제
blueorbit.tistory.com
https://blueorbit.tistory.com/36
Renal replacement therapy을 언제 중단할 수 있을까
Renal replacement therapy(투석)이 더 필요하지 않다고 판단하여 중단하는 경우는, 환자의 신장 기능이 환자의 체내 요구에 충분할 만큼 회복되었거나, 치료 목표를 달성하는데 더 이상 필요하지 않은
blueorbit.tistory.com
'의학' 카테고리의 다른 글
| KDIGO Clinical Practice Guidelines for Acute Kidney Injury_1 (0) | 2024.02.26 |
|---|---|
| 중증 패혈증 환자에서 베타 락탐 항생제의 지속적 주입 용법과 간헐적 주입 용법의 비교 (1) | 2024.02.25 |
| Teicoplanin (0) | 2024.02.25 |
| 비만 환자에서 항생제 용량을 계산할 때 고려사항 (1) | 2024.02.24 |
| 장폐색(ileus)의 발생 기전 (0) | 2024.02.24 |



