When Should a NOAC Be Withheld Befor Surgery?
수술 전후 기간 동안 NOAC를 언제 일시적으로 중단할지 여부는 다음 2 가지 사항을 고려해야 한다.
(1) 시술 혹은 수술의 출혈 위험성 정도
(2) 환자의 신장 기능을 고려했을 때 예상되는 NOAC 제거 시간
이론적으로 NOAC를 갑자기 중단한다면 stroke 위험성이 높아질 것으로 생각되지만, 여러 major NOAC trial의 washout period에 대한 연구에 따르면, NOAC의 중단으로 storke의 정상적인 off-treatment risk의 재개가 이루어지고 이는 'rebound' prothrobic state가 아닌 것으로 알려졌다.
Patel MR et al; ROCKET AF Investigators. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011; 365(10):883-891.
수술을 위해 NOAC를 며칠간 중단했을 때 thrombotic event 발생의 위험성은 대부분의 환자에서 작다.
Bleeding Risk of the Procedure
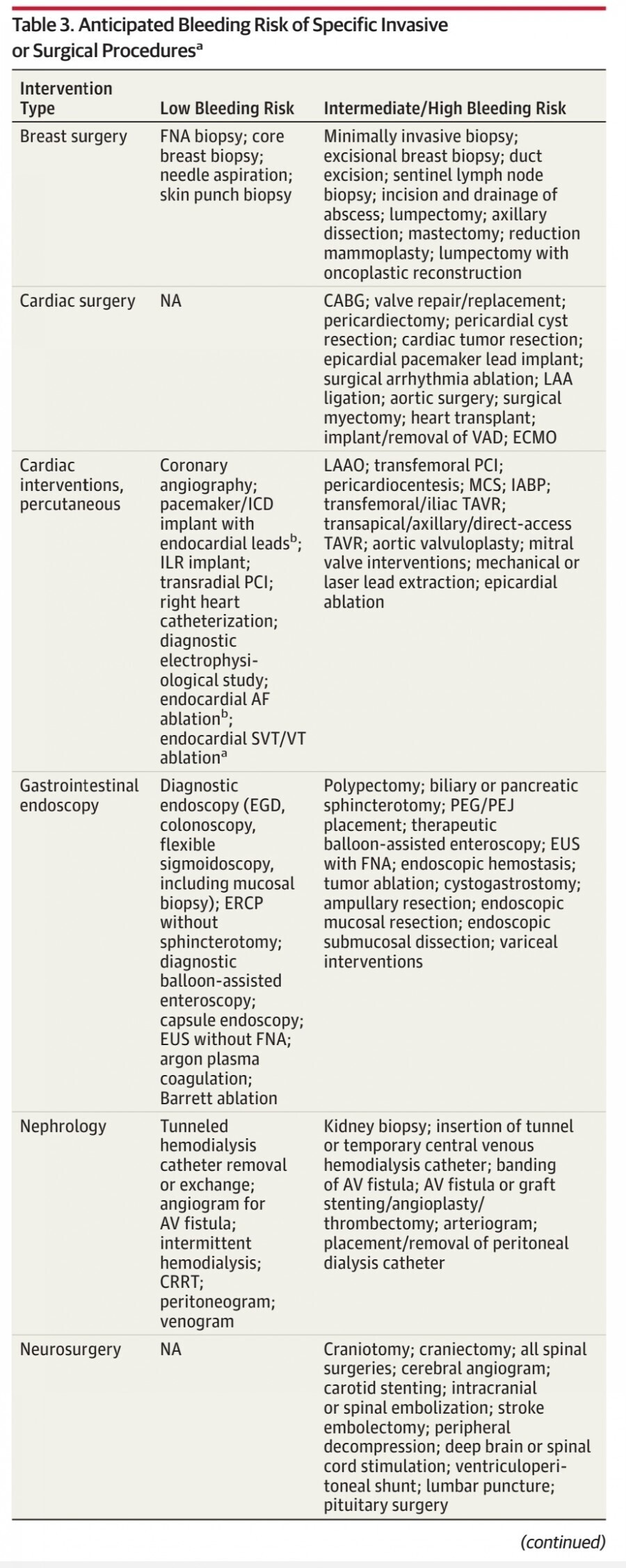
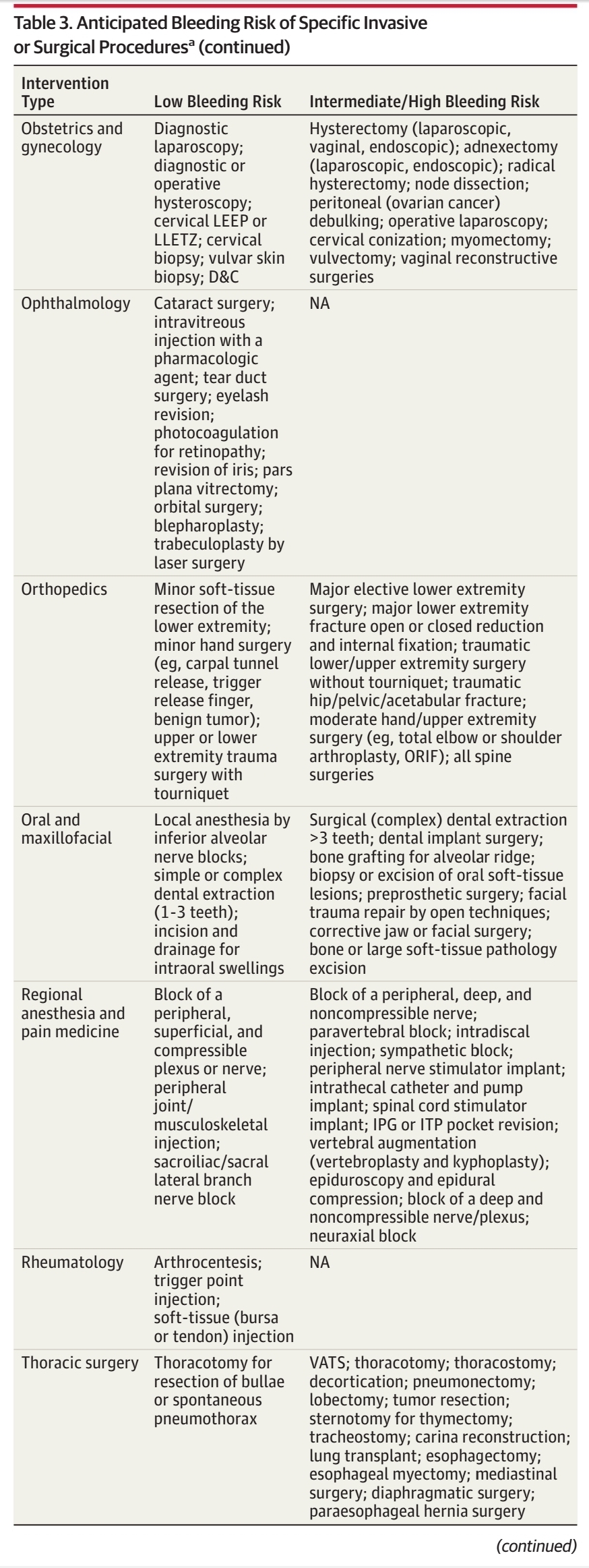

Bleeding risk of a given procedure
Minimal, low: 2 day risk of bleed, < 2%
Intermediate/high: 2 day risk of bleed, ≥ 2%
Low or minimal bleeding risk에 해당하는 수술을 할 때,
NOAC를 수술 24시간 전부터 중단해도 안전하며, 수술 당시 residual anticoagulant effect가 12~25% 정도라면 심한 출혈 위험은 낮다고 알려져 있다.
Verma A et al; CCS Atrial Fibrillation Guidelines Committee. 2014 Focused update of the Canadian Cardiovascular Society Guidelines for the management of atrial fibrillation [published corrections appear in Can J Cardiol. 2014;30(12):1495 and 2015;31(10):1302]. Can J Cardiol. 2014;30(10):1114-1130.
몇 가지 시술들은 NOAC 중단 없이 시행할 수 있다:
- simple or superficial dermatologic excisions or biopsies
- simple cataract and glaucoma surgical procedures
- minor dental procedures that include extraction of 1 or 2 teeth
- gastrointestinal endoscopy without biopsy
이 시술들은 trough NOAC drug level을 고려해서 시행할 수 있다. 하지만, 이와 같은 uninterrupted NOAC therapy에 대한 무작위 연구는 매우 제한적이며, 주로 catheter based AF ablation에 대한 연구에 기반하고 있다.
Calkins H et al; RE-CIRCUIT Investigators. Uninterrupted dabigatran versus warfarin for ablation in atrial fibrillation. N Engl J Med. 2017;376(17):1627-1636.
Intermediate or high bleeding risk에 해당하는 수술을 할 때는, residual anticoagulant effect가 10% 미만으로 존재해야 하며, NOAC는 수술 48시간에서 72시간 전에 중단해야 한다. Pivotal NOAC trial에 따르면 NOAC interruption 그룹과 warfarin interruption 그룹( 'bridging' 여부에 상관없이) 간에 thromboembolism이나 bleeding rate는 유의한 차이가 없었다.
Sunkara T, Ofori E, Zarubin V, CaugheyME, Gaduputi V, Reddy M. Perioperative management of direct oral anticoagulants (DOACs): a systemic review. Health Serv Insights. 2016;9(suppl 1):25-36.
Dabigatran과 warfarin을 비교한 Randomized Evaluation ofLong-term Anticoagulation Therapy(RE-LY) study에서는 perioperative 30-day bleeding rate이 3%, thromboembolic rate가 0.5% 발생하였다.
Douketis JD et al. Urgent surgery or procedures in patients taking dabigatran or warfarin: analysis of perioperative outcomes from the RE-LY trial. Thromb Res. 2016; 139:77-81.
In the Rivaroxaban Once Daily, Oral, Direct Factor Xa Inhibition Compared With Vitamin K Antagonism for Prevention of Stroke and Embolism Trial in Atrial Fibrillation (ROCKETAF) study에서는 periopeartive thromboembolic risk가 rivaroxaban 그룹에서 0.3%, warfarin 그룹에서 0.4% 발생하였다.
Sherwood MW et al; ROCKET AF Investigators. Outcomes of temporary interruption of rivaroxaban compared with warfarin in patients with nonvalvular atrial fibrillation: results from the Rivaroxaban Once Daily, Oral, Direct Factor Xa Inhibition Compared With Vitamin K Antagonism for Prevention of Stroke and Embolism Trial in Atrial Fibrillation (ROCKET AF). Circulation. 2014;129(18):1850-1859. 35.
Apixaban for Reduction in Stroke and Other Thromboembolic Events in Atrial Fibrillation (ARISTOTLE) trial에서는, 수술 전후에 apixaban을 중단한 군과 계속 복용한 군을 비교하였는데 major bleeding과 thromboembolism이 모두 유의하게 낮았다고 발표하였다.
Garcia D, Alexander JH, Wallentin L, et al. Management and clinical outcomes in patients treated with apixaban vs warfarin undergoing procedures. Blood. 2014;124(25):3692-3698. 36.
Neuraxial (spinal or epidural) anesthesia는 매우 심각한 결과를 초래할 수 있는 spinal or epidural hematoma의 위험성이 있는 시술로서, high-risk surgery와 같은 NOAC 중단 가이드라인을 따라야 한다.
American Society of Regional Anesthesia and Pain Medicine의 가장 최근 가이드라인에서는 spinal or epidural anesthesia 예정 시에 dabigatran은 4일에서 5일 전에 중단하고, apixaban과 rivaroxaban은 최소 3일 전에 중단할 것을 권고하고 있다.
다른 high-risk surgical procedure에 비해 중단 기간이 다소 길지만, 이는 spinal instrumentation surgery 전에 최소 5 half-lives에 해당하는 기간 동안 중단하는 근거에 따랐다. 이러한 권고들은 paravertebral block과 sympathetic block과 같은 intermediate risk pain procedure에도 적용할 수 있다. Peripheral nerve and sacral lateral branch block은 low risk이며, 가이드라인에서는 2 half-lives 동안 중단할 것을 권고하고 있다; 하지만, 이 가이드라인은 expert recommendation에 기반하고 있으며, clinicaltiral data가 아님을 유념해야 한다.
Narouze S et al. Interventional spine and pain procedures in patients on antiplatelet and anticoagulant medications: guidelines from the American Society of Regional Anesthesia and Pain Medicine, the European Society of Regional Anaesthesia and Pain Therapy, the American Academy of Pain Medicine, the International Neuromodulation Society, the North American Neuromodulation Society, and the World Institute of Pain. Reg Anesth Pain Med. 2015; 40(3):182-212.
NOAC Clearance in the Setting of Abnormal Kidney Function
신장 기능이 정상(CrCl > 50 mL/min)인 환자에서는 NOAC를 48시간 동안 중단했을 때 residual anticoagulant effet는 10% 미만(equivalent to 3-4 half-lives ) 남아 있게 된다. Dabigatran은 대부분 renal clearance에 의해 제거되므로(대략 80%), FXa inhibitor과 서로 다른 방법으로 접근해야 한다.
CrCl 30~50 mL/min인 환자가 FXa inhibitor 복용 중이라면 수술 48시간 전에 약을 중단해야 하지만, daibitran은 residual anticoagulant effet를 최소화하기 위해 추가로 24시간에서 48시간을 더 중단해야 한다.
Gunasekaran P et al. Periprocedural management of non–vitamin K oral anticoagulants in chronic kidney disease: a review of existing heterogeneity and contemporary evidence. JAtr Fibrillation. 2015;8(4):1230.
중증의 만성 신부전 환자(CrCl, 15-29mL/min)가 FXa inhibitor를 복용 중이었다면, invasive procedure 최소 72시간 전에 복용을 중단해야 하고, dabigatran 복용 환자는 96시간에서 120시간 전에 중단해야 한다.
Doherty JU et al. 2017 ACC Expert Consensus Decision Pathway for Periprocedural Management of Anticoagulation in Patients With Nonvalvular Atrial Fibrillation: a report of the American College of Cardiology Clinical Expert Consensus Document Task Force. J AmColl Cardiol. 2017;69(7):871-898. 20.
CrCl < 15mL/min이거나 혈액 투석을 받는 신부전 환자에서는
NOAC 복용을 추천하지 않는다.
Reference
What Surgeons Should KnowAbout Non–Vitamin K Oral Anticoagulants: A Review
JAMA Surg. 2018;153(6):577-585.
2021.11.04 - [의학] - 복부 둔상 환자에서 항응고 치료는 언제 시작해야 할까?
복부 둔상 환자에서 항응고 치료는 언제 시작해야 할까?
Hypercagulability Following Blunt Solid Abdominal Organ Injury: When to Initiate Anticoagulation Background 둔상(blunt trauma)으로 인해 복강 내 장기 손상을 입은 환자에서 venous thromboembolism(정맥 혈전색전증) 예방을 위한
blueorbit.tistory.com
2021.11.07 - [의학] - NOACs 복용 환자가 수술 시 heparin 사용 여부와 NOACs 재복용 시점
NOACs 복용 환자가 수술 시 heparin 사용 여부와 NOACs 재복용 시점
Do I Need to Bridge Patients With Heparin When Therapy With NOACs Is Withheld? 일시적으로 NOAC 복용을 중단해야 할 때, 수술 전후 동안 heparin sodium으로 bridging 하는 것은 추천하지 않는다. 대부분의 환자에서 NOAC 복
blueorbit.tistory.com
2021.11.12 - [의학] - 수술 환자에서 NOACs 대신 warfarin을 복용해야 하는 경우는?
수술 환자에서 NOACs 대신 warfarin을 복용해야 하는 경우는?
Non-vitamin K oral anticoagulants(NOACs) Non-vitamin K oral anticoagulants(NOACs)는 nonvalvular atrial fibrillation(AF) 환자에서 thromboembolism(혈전색전증)의 예방과, deep vein thrombosis(DVT, 심부정맥 혈전증)와 pulmonary embolism(PE,
blueorbit.tistory.com
'의학' 카테고리의 다른 글
| Machine learning을 이용한 패혈증 환자의 Simple Weaning Model (0) | 2022.05.21 |
|---|---|
| NOACs을 복용 중이던 환자가 응급 수술을 받는 경우 (0) | 2021.11.15 |
| 수술 환자에서 NOACs 대신 warfarin을 복용해야 하는 경우는? (0) | 2021.11.12 |
| Solute(용질)의 concentration을 나타내는 단위와 electroneutrality(전기적 중성) (0) | 2021.11.07 |
| Body fluid compartment(체액 구획)에서 수분의 분포 (0) | 2021.11.07 |


