Delirium 발생에 대한 pathophysiology
Delirium(섬망) 발생에 대한 병태생리학적 기전은 아직 완전히 밝혀지지 않았지만, 다음 세 가지 기전이 가설로 제시된다.
1. Neurotransmitter imbalance
dopamine (과잉), acetylcholine (상대적인 결핍), γ-aminobutyric acid (GABA), serotonin, endorphins, norepinephrine, glutamate와 같은 여러 neurotransmitter(신경 전달 물질)이 관련되어 있다.
2. Inflammatory mediators
Tumor necrosis factor alpha (TNF-α), interleukin-1 (IL-1), 및 기타 cytokines, chemokines와 같은 inflammatory mediators는 CNS의 endothelial damage, thrombin formation, microvascular dysfunction의 발병 기전과 관련이 있으며, 이는 delirium 발병에 기여한다. 최근 여러 연구에서 delirium의 기간을 증가시키는 데 endothelial dysfunction이 기여한다는 결과들이 보고되고 있다.
3. Impaired oxidative metabolism.
이 가설에 따르면, oxydative metabolim의 global failure에 대한 이차적인 cerebral insufficiency의 결과로 delirium이 발생할 수 있다.
4. Large neutral amino acids
Tryptophan과 tyrosine의 증가된 cerebral uptake의 결과로 CNS에서 serotonin, dopamine, norepinephrine의 농도가 증가하게 된다. 이러한 amino acids의 availability 변화는 delirium 발생 위험 증가와 관련되어 있다.
2024.01.21 - [의학] - 섬망의 정의와 위험 인자
섬망의 정의와 위험 인자
Delirium(섬망)의 정의 1. 집중, 유지, 또는 주의를 전환하는 능력이 감소된 의식 장애(disturbance of consciousness). 즉, 주변 환경에 대한 인식의 명확성이 감소. 2. 인지(cognition) 능력의 변화(eg, memory defici
blueorbit.tistory.com
Delirium 평가 방법
Society of Critical Care Medicine (SCCM)에서는 pain, anxiety, delirium에 대해 routine monitoring을 시행하고 이러한 condition에 대한 치료에 대한 반응을 기록할 것을 권고하고 있다. Agitation(진전)과 delirium을 평가하는 여러 진단 도구가 있다: Ramsay Scale, Riker Sedation-Agitation Scale (SAS), Motor Activity Assessment Scale (MAAS), Richmond Agitation-Sedation Scale (RASS), Adaptation to Intensive Care Environment (ATICE) scale, Minnesota Sedation Assessment Tool (MSAT)
이러한 척도 대부분은 성인 중환자에서 우수한 reliability와 validity를 보이며 goal-directed sedative administration의 목표를 설정하는 데 사용할 수 있다. Sedation-Agitation Scale (SAS)는 평가자 간 reliability(kappa = 0.92)가 우수하고 다른 척도와도 높은 correlation(상관관계, r2 = 0.83 to 0.86 )를 나타낸다. Richmond Agitation-Sedation Scale (RASS)는 시간에 따른 의식 수준의 변화를 확인하거나 진정제나 진통제 투여 후 반응을 확인할 수 있는 유일한 척도이며, agitation과 delirium의 정도를 평가할 수 있다.

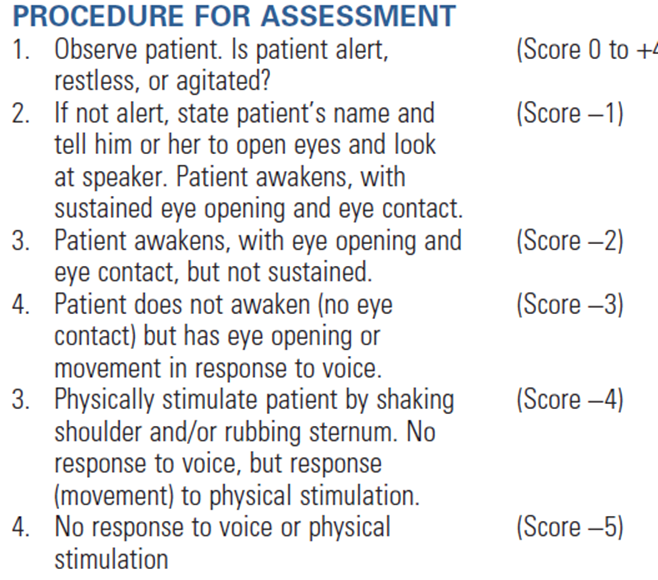
환자 평가는 3단계로 이루어진다.
1. 먼저 환자의 alert, restless, agitated를 평가한다(0 ~ +4).
2. 환자가 alert하지 않고 positive motoric characteristics를 보이지 않는다면, 환자의 이름을 불러보고 eye contact 시간을 확인함으로써 sedation level을 평가한다(-1 ~ -3).
3. Verbal stimulation에도 환자가 눈을 뜨지 않는다면 어깨를 흔들거나 흉골을 누르는 등의 자극을 가하고 그 반응 여부를 기록한다(-4 ~ -5).
이러한 평가를 완료하는 데 20초도 걸리지 않으며, 진정의 다른 평가(eg, Glasgow Coma Scale [GCS], bispectral electroencephalography, neuropsychiatric ratings)와도 연관성이 높은 것이 장점이다. 예전에는 중환자에서 발생하는 delirium을 평가하는 타당하고 신뢰할 수 있는 방법이 없었는데, 중환자들이 sedative agents를 투여받고 있거나 혹은 mechanical ventilation 중이라면 말로 표현할 수 없는 것이 그 이유였다. 하지만 최근에는 intubation 되어 있는 환자들에게도 적용이 가능하고 Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria에 따라 평가 가능한 여러 진단 방법들이 개발되었다. Confusion Assessment Method for the ICU (CAM-ICU)와 Intensive Care Delirium Screening Checklist (ICDSC)가 대표적인 도구이다.
Confusion Assessment Method for the ICU (CAM-ICU)
중환자의학과, 정신건강의학과, 신경과 및 노인의학 전문가 팀이 개발한 delirium 측정 도구인 CAM-ICU는 간호사가 수행할 수 있으며, 평가에 1 ~ 2분밖에 걸리지 않는다.
그리고 정신건강의학과 전문의가 DSM-V를 기반으로 평가한 방법과 비교해서 delirium을 진단할 확률이 98% 일 정도로 정확한 진단 도구이다.
CAM-ICU를 시행하기 위해 먼저 환자의 의식 수준을 확인하고, verbal command에 반응하는 환자(RASS score -3 점 이상의 각성 수준)는 delirium 평가를 시작할 수 있다.

CAM-ICU는 네 가지 특징을 갖고 있다:
1. Mental status가 baseline으로부터 변화하는 경우 혹은 mental status의 fluctuation
2. Inattension
3. Disorganized thinking
4. altered level of consciousness
환자가 1, 2번 특징을 모두 갖고 있고, 3번과 4번 중 한 가지를 갖고 있다면 delirium으로 진단할 수 있다.
Intensive Care Delirium Screening Checklist (ICDSC)
ICDSC는 inattention, disorientation, hallucination, delusion or psychosis, psychomotor agitation or retardation, inappropriate speech or mood, sleep/wake cycle disturbances 및 이러한 증상의 fluctuation을 평가하는 checklist 기반 평가 도구이다.
8개의 항목은 각각의 유무(0 또는 1)로 점수를 매기고 합산하며, 4점 이상이면 delirium이 있음을 나타내고 0점은 없음을 나타낸다.
1 ~ 3점 사이인 환자는 subsyndromal delirium이 있는 것으로 간주되며, 이는 delirium이 없는 환자보다 더 나쁜 예후를 보이지만 확실히 진단되는 delirium과 비교해서는 더 나은 예후를 보인다.

최근 한 연구는 sedation 상태 환자에 대한 delirium 평가의 유용성에 의문을 제기하였다.
Patel SB et al. Rapidly reversible, sedation-related delirium versus persistent delirium in the intensive care unit. Am J Respir Crit Care Med 2014;189(6):658– 665.
Haenggi M, Blum S, Brechbuehl R, Brunello A, Jakob SM, Takala J. Effect of sedation level on the prevalence of delirium when assessed with CAM-ICU and ICDSC. Intensive Care Med 2013; 39(12):2171-2179.
이 연구에서는 소수의 환자(약 10%)가 빠르게 회복되는 sedation-related delirium을 진단받았지만, 이 중 대부분인 sedation 중단 후에도 persistent delirium을 보였다. 이 결과를 따른다면 가능한 경우 sedation을 중단한 후 delirium 평가를 시행해야 하겠지만, 몇몇 환자에서는 delirium을 overdiagnosis 하는 것이 진단을 놓치는 것보다 덜 해로울 것이기 때문에 sedation 중이라고 해서 delirium 평가를 생략해서는 안 된다.
Reference
Chapter 2. Agitaion and Delirium. Textbook of critical care, 7th ed. Elsevier
2022.07.01 - [의학] - 섬망의 예방과 치료
섬망의 예방과 치료
Delirium(섬망)의 예방 및 치료에 대한 효과적인 evidence-based strategies와 protocol의 개발을 위해 현재 비약리학적 및 약리학적 접근에 대한 여러 건의 RCT가 진행되고 있다. 안정적이었던 환자에서 agitat
blueorbit.tistory.com
2024.02.18 - [의학] - Delirium(섬망)의 약물적 예방 및 치료
Delirium(섬망)의 약물적 예방 및 치료
현재 섬망의 치료에 임상적으로 사용하는 약물로는 전형적인 항정신병제(haloperidol), 비정형 항정신병제 (risperidone, olanzapine, quetiapine) 그리고 dexmedetomidine 등이 있다(표 9). 섬망의 약물치료 섬망을
blueorbit.tistory.com
'의학' 카테고리의 다른 글
| ICU-acquired weakness 위험 인자 및 영향 (0) | 2022.07.04 |
|---|---|
| 섬망의 예방과 치료 (0) | 2022.07.01 |
| Monitoring nutritional support (0) | 2022.06.20 |
| Lactate은 외상 환자의 병원전 단계에서 plasma 수혈의 효과를 보여준다 (0) | 2022.06.19 |
| Sepsis-induced DIC 환자에서 antithrombin을 언제 투여해야 할까? (0) | 2022.06.08 |



